

 Print | Share
Print | Share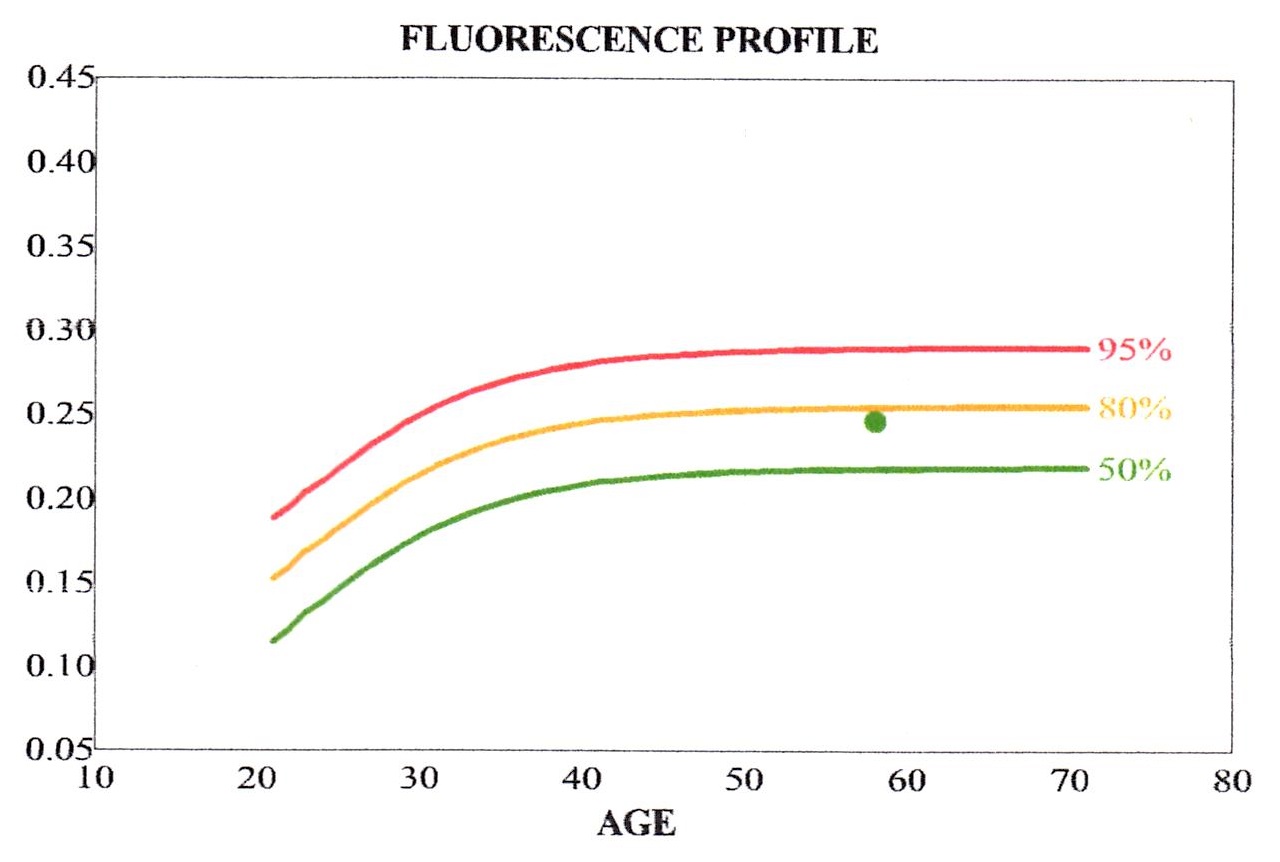 Elevated lens autofluorescence is a
Elevated lens autofluorescence is a
biomarker of diabetes
ICD-10 Diagnosis Code:
E11.3 — Type 2 Diabetes with Ophthalmic Complications
Title
Diabetes with Ophthalmic Manifestations
Category
Diabetes Mellitus
Description
Diabetes mellitus s a complex, multifactorial and heterogenous group of disorders characterized by insulin deficiency and/or insulin resistance.
Diabetes
Diabetes mellitus is a complex, multifactorial and heterogeneous group of disorders characterized by endogenous insulin deficiency and/or insulin resistance. The disease manifests itself as a state of chronic hyperglycemia with attendant microvascular and macrovascular complications.
Diabetes with Ophthalmic Manifestations
Diabetes produces many ophthalmic manifestations. A disease manifestation is an expression or an associated disorder of a disease process, but is not the primary disease. Diabetes can produce the following ophthalmic manifestations.
Refractive Changes
Diabetes causes the glucose and sorbitol levels in the body to fluctuate. As these levels fluctuate, they have the ability to affect the tonicity of the crystalline lens in the eye. Significant changes in the lens tonicity can cause the lens to shrink or swell. These changes in lens shape produce changes in the lens curvature that alter the refractive power of the eye.
Glaucoma
Diabetes is an important cause in about 32% of patients with neovascular glaucoma. This type of neovascular glaucoma, known as diabetic glaucoma, is caused by iris neovascularization that occludes the trabecular meshwork of the anterior chamber.
Cataracts
Diabetes may produce an osmotic shock in the crystalline lens which produces bilateral white punctate or snowflake opacities. In some cases, diabetic cataracts can mature in a few days.
Cranial Nerve Palsies
Vascular diseases such as diabetes or hypertension are the most common cause of a pupil-sparing third nerve palsy. The palsy is thought to be caused by a demyelinization of the nerve, with spontaneous recovery usually occurring within three months. Diabetic third nerve palsy are often associated with periorbital pain and are occasionally the presenting feature of diabetes.
Diabetic Retinopathy
This is the most common and most serious ophthalmic manifestation of diabetes mellitus. It is a microangiopathy affecting the retinal blood vessels, and has features of both microvascular occlusion and leakage.
Diabetes is a disease in epidemic proportion in the United States. In 2012, it is estimated that approximately 26 million people in the United States are diabetic and another 79 million are pre-diabetic. Dramatic increases in disease prevalence are expected.
In addition to the significant array of systemic complications associated with diabetes, ocular complications are common.
- Diabetic changes in the retina occur 60% of the time in diabetics presenting with more than a 10 year history of the disease
- This increases to 80% at 15 years with 25% developing proliferative changes at this point
The main goal of the diagnostic evaluation in a patient with diabetes is to accomplish the following:
- Determine the presence or absence of diabetic retinopathy
- Classify the diabetic retinopathy
- Identify and exclude differential diagnosis
- Determine if the retinopathy is clinically significant and/or vision threatening
- Prescribe a treatment program
Symptoms of Type 2 diabetes can appear slowly. Some patients do not notice symptoms at all. The symptoms can include:
- Excessive thirst
- Excessive urination
- Feeling very hungry or tired
- Losing weight without trying
- Having sores that heal slowly
- Blurry or fluctuating vision
Patient History
The severity of the symptoms or signs is varied and depends on the level of control the patient has over their diabetes. Patients can present with the following abnormal symptoms:
- Blurred vision (sudden or gradual)
- Distorted vision (sudden or gradual)
- Difficulty driving at night
- Floaters or dark spots in their field of view
Clinical Appearance of the Crystalline Lens
- Glycosylated end products accumulate in the crystalline lens in the presence of diabetes and uncontrolled glucose
- Elevated autofluorescence measurements have been linked to high levels of advanced glycosylated end products
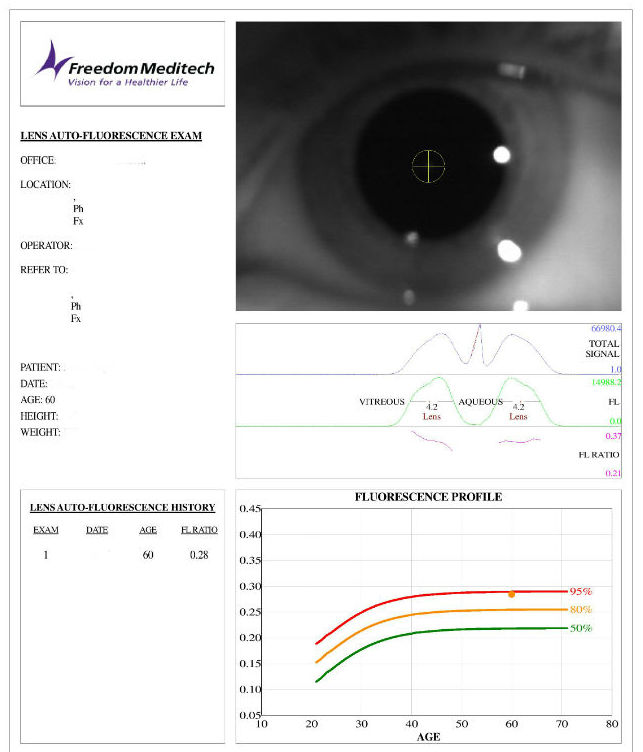
- The lens fluorescence ratio can be measured with the Clearpath DS-120 Lens Fluorescence Biomicroscope from Freedom Meditech
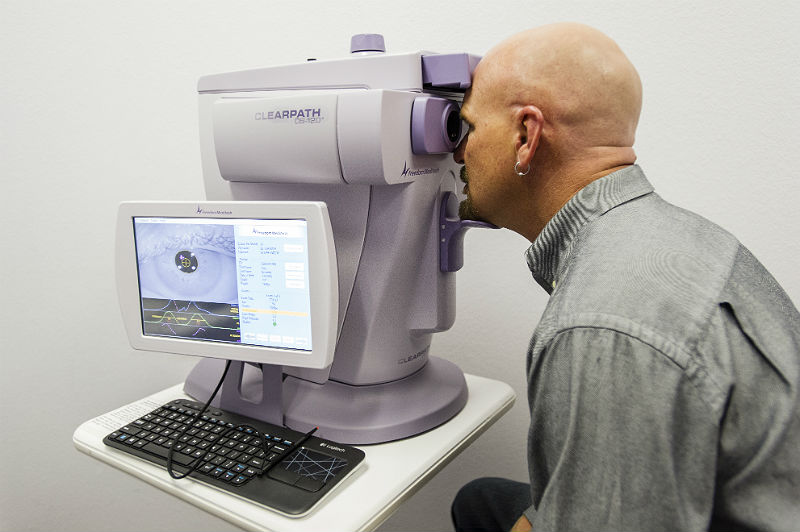 |
Lens Fluorescence Biomicroscope
|
|
Fluorescence Profile
|
 |
Clinical Appearance of the Retina
The retinal changes associated with diabetic retinopathy include the following:
- Hemorrhages
- Microaneurysms
- Lipid deposits
- Cotton wool spots
- Edema
- Ischemia
- Venous beading
- Intraretinal microvascular abnormalities
- Retinal thickening
- Neovascularization
- Proliferative non-inflammatory degeneration
DIAGNOSTIC TESTS
Fundus Photography
- To document the progress or lack of progress of diabetic retinopathy
- To document the delivery of medical treatment
- To document the response to treatment
- To help plan a treatment program
- Fundus autofluorescence imaging can be used to detect structural abnormalities and predict functional deficits before standard color fundus photography
- Multi-spectral imaging with the Annidis RHA System can be used to detect structural abnormalities and predict functional deficits before standard color fundus photography
Retinal Scanning Laser
- To measure the microscopic anatomy of the retina and vitreoretinal interface
- To measure the effectiveness of therapy
- To help in determining the need for ongoing therapy
- To determine the safety of cessation of therapy
Visual Field Examination
- Used to assess visual function and determine the size of any associated visual field defects
- Visual field may be affected depending on the size and location of retinal hemorrhaging the extent of the visual field defect depends on size of macular edema
B-Scan Ophthalmic Ultrasound
- A two-dimensional ultrasonic scanning procedure used to produce cross-sectional images of the eye and orbit
- B-scan ophthalmic ultrasound can be used to assess internal structures of the eye when a vitreous hemorrhage prevents proper visualization and examination of the retina
- The test results are used to determine whether the retina is attached or detached
Although there are several types of diabetes, depending on patient circumstances, there are two main classifications that most can be included in. They are:
Type I Diabetes
- Results from a cullular-mediated autoimmune destruction of the B-cells of the pancreas
- Usually leads to absolute insulin deficiency
- Accounts for 5-10% of diabetics nationwide
- Some patients, particularly children and adolescents, may present with ketoacidosis as the first manifestation of the disease
- Other patients have modest fasting hyperglycemia that can rapidly change to severe hyperglycemia and/or ketoacidosis in the presence of infection or other stress
- Still others, particularly adults, may retain residual B-cell function sufficient to prevent ketoacidosis for many years; such individuals eventually become dependent on insulin for survival and are at risk for ketoacidosis
- Immune-mediated diabetes commonly occurs in childhood and adolescence, but it can occur at any age, even in the 8th and 9th decades of life
Idiopathic Diabetes
Some forms of type I diabetes have no known etiologies. Some of these patients have permanent insulinopenia and are prone to ketoacidosis, but have no evidence of autoimmunity. Although only a minority of patients with type I diabetes fall into this category, of those who do, most are of African or Asian ancestry. Individuals with this form of diabetes suffer from episodic ketoacidosis and exhibit varying degrees of insulin deficiency between episodes. This form of diabetes is strongly inherited and lacks immunological evidence for B-cell autoimmunity. An absolute requirement for insulin replacement therapy in affected patients may come and go.
Type II Diabetes
- Referred to as non-insulin-dependent diabetes, it encompasses individuals who have insulin resistance and usually have relative (rather than absolute) insulin deficiency
- At least initially, and often throughout their lifetime, these individuals do not need insulin treatment to survive
- Accounts for 90-95% of diabetics nationwide
- Autoimmune destruction of B-cells does not occur
- Most patients with this form of diabetes are obese, and obesity itself causes some degree of insulin resistance
- Ketoacidosis seldom occurs spontaneously in this type of diabetes; when seen, it usually arises in association with the stress of another illness such as infection
- Frequently goes undiagnosed for many years because the hyperglycemia develops gradually and at earlier stages is often not severe enough for the patient to notice any of the classic symptoms
- Insulin secretion is defective in these patients and insufficient to compensate for insulin resistance. Insulin resistance may improve with weight reduction and/or pharmacological treatment of hyperglycemia but is seldom restored to normal
- The risk of developing this form of diabetes increases with age, obesity, and lack of physical activity
Correctly determining whether a patient has type 1 or type 2 diabetes is important because patients with type 1 diabetes require continuous exogenous insulin for survival. In contrast, treatment of type 2 diabetes consists of lifestyle measures and a variety of other medications, with insulin introduced if those prove inadequate.
As previously stated, patients with type 2 diabetes mellitus can usually be differentiated from those with type 1 disease on the basis of history and physical examination findings and through simple laboratory tests. Patients with type 2 diabetes are generally obese, and may have acanthosis nigricans and/or hirsutism in conjunction with thick necks and chubby cheeks.
A patient whose diabetes has been controlled with diet or an oral antidiabetic agent for longer than several months generally has type 2 diabetes. A lean patient who has had diabetes since childhood, who has always been dependent on insulin, or who has a history of diabetic ketoacidosis (DKA) almost certainly has type 1 diabetes.
When dealing with patients with known diabetes in the emergency department, distinguishing the type of diabetes can be difficult in 2 groups: (1) patients who are treated with insulin and are young but clinically appear to have type 2 diabetes, and (2) older patients with late-onset of diabetes who nonetheless take insulin and seem to share characteristics of patients with type 1 diabetes.
Prediabetes
Prediabetes often precedes overt type 2 diabetes. Prediabetes is defined by a fasting blood glucose level of 100-125 mg/dL or a 2-hour post-oral glucose tolerance test (post-OGTT) glucose level of 140-200 mg/dL. Persons with prediabetes are at increased risk for macrovascular disease, as well as diabetes.
Often confused with prediabetes is the metabolic syndrome (also called syndrome X or the insulin-resistance syndrome). Metabolic syndrome, thought to be due to insulin resistance, can occur in patients with overtly normal glucose tolerance, prediabetes, or diabetes. It is diagnosed when a patient has at least 3 of the following 5 conditions:
-
Abdominal obesity
-
Elevated triglyceride level
-
Low level of high-density lipoprotein (HDL) cholesterol
-
Elevated blood pressure
-
Fasting glucose value of 100 mg/dL or higher
Eventually, clinically apparent insulin resistance develops. Unfortunately, insulin resistance is not possible to measure clinically, except in research settings. An elevated fasting blood glucose or triglyceride level may be the first indication of insulin resistance. Fasting insulin levels are generally increased at an earlier stage, but they are more directly related to insulin clearance than to insulin resistance. An effort to standardize insulin assays is under way and may allow for the use of fasting insulin levels to diagnose insulin resistance in the future.
Although optometrists and ophthalmologists do not treat diabetes directly, the role of the primary eye care provider cannot be over-emphasized in the management of the diabetic patient.
- Healthy eating
- Physical activity
- Blood glucose testing
- Oral medications
- Insulin
1. Negi A, Vernon S. An overview of the eye in diabetes. National Center for Biotechnology Information. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC539505/. Last accessed January 8, 2015.
2. Skarbez K, Priestley Y, Hoepf M, Koevary S. Comprehensive review of the effects of diabetes on ocular health. Medscape. Expert Rev Ophthalmol. 2010;5(4):557-577. http://www.medscape.com/viewarticle/729120. Last accessed January 8, 2015.
3. Diagnosis and Classification of Diabetes Mellitus. American Diabetes Association. Jan 2004. http://care.diabetesjournals.org/content/27/suppl_1/s5.full. Last accessed January 18, 2015.
4. Risk Factors For Diabetes. WebMD. http://www.webmd.com/diabetes/risk-factors-for-diabetes. Last accessed January 20, 2015.
250.50
Diabetes with ophthalmic manifestations,
type II or unspecified type, not stated as uncontrolled
92015
Refraction
Occurence
- The prevalence of diabetic retinopathy among diabetic patients is 8.2% of the population over the age of 40 years old
Distribution
- Diabetic retinopathy is not distributed evenly throughout the population
Risk Factors
Crystalline Lens Autofluorescence
- The fluorescence ratio of the crystalline lens increase with the incidence of diabetes and/or uncontrolled blood glucose
Type I Diabetes
- Genetics and family history
- Diseases of the pancreas
- Infection or illness
Type II Diabetes
- Obesity or being overweight
- Impaired glucose tolerance
- Insulin resistance
- Ethnic background
- High blood pressure
- History of gestational diabetes
- Sedentary lifestyle
- Family history
- Polycystic ovary syndrome
- Age