

 Print | Share
Print | Share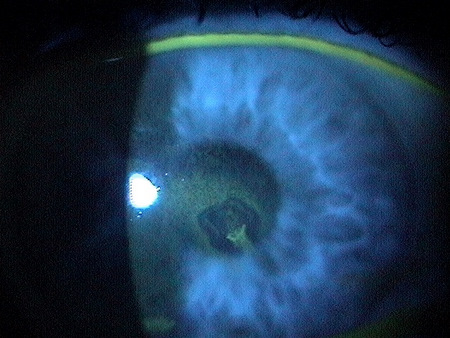
Recurrent erosion of the cornea in the pupillary zone
ICD-10 Diagnosis Codes:
H18.831–Recurrent erosion of cornea, right eye
H18.832–Recurrent erosion of cornea, left eye
H18.833–Recurrent erosion of cornea, bilateral
Title
Recurrent Erosion of Cornea
Category
Corneal Opacity And Other Disorders Of Cornea
Description
A corneal erosion is characterized by a spontaneous detachment of the basal cells of the corneal epithelium from the underlying basement membrane.
Corneal Erosion
- Occurs when there is a weak attachment between the basal cells of the corneal epithelium and Bowman’s membrane
- When a weak attachment is present, shearing forces produced by the eyelids or minor friction across the cornea can cause movement or sloughing of the epithelium
Recurrent Corneal Erosion
- If the condition occurs after a history of corneal trauma or if it occurs more than once, it is called recurrent corneal erosion
In many cases of recurrent cornea erosion, patients have a history of corneal abrasion in the involved eye, often months or years previously.
The mechamical trauma often involves organic structures like plants and fingernails. One theory is that particulate matter or oils on these surfaces remain attached to the exposed basement membrane, creating a potentially permanent barrier to true attachement of the epithelium to the basement membrane.
The original trauma that produced the corneal abrasion also damages the attachment structures between the corneal epithelium and the underlying basement membrane. While the two layers can be in apposition after the injury, they are not truly attached. Every time the layers are pulled apart, the area of damaged attachement can grow. Other causes of recurrent corneal erosion include pre-existing corneal disease and ocular surgery.
One of the major sources of recurrent corneal erosion is a corneal abrasion that was not aggressively treated. Abrasions with rough edges, epithelial tags, edema at the edge of the abrasion, areas of rolled epithelial edges and visible debris on the exposed basement membrane are all predictors for future erosion problems. These wounds should be debrided or, even better, treated with a diamond burr to contour the edges of the abrasion and create a smooth basement membrane. This simple step will eliminate a many future erosions.
Structural Damage to the Eye
- Epithelial sloughing
- Corneal edema
 |
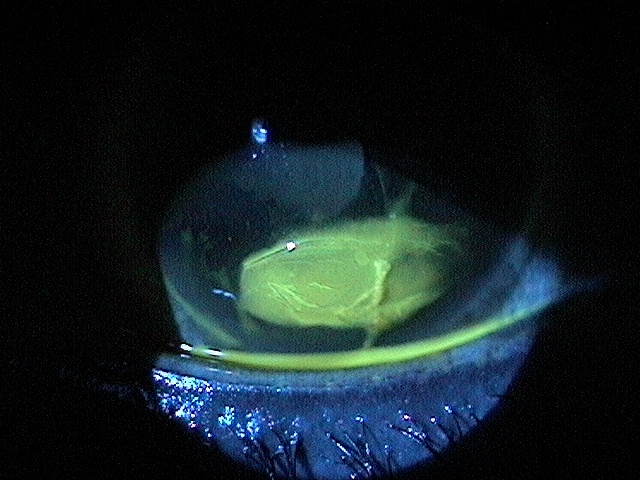
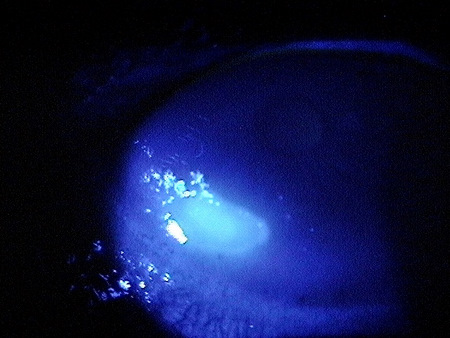
Corneal Laceration – Day 1
|
|
 |
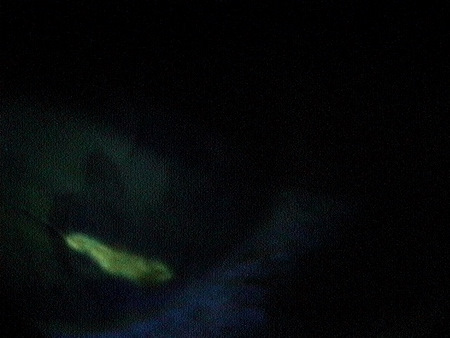
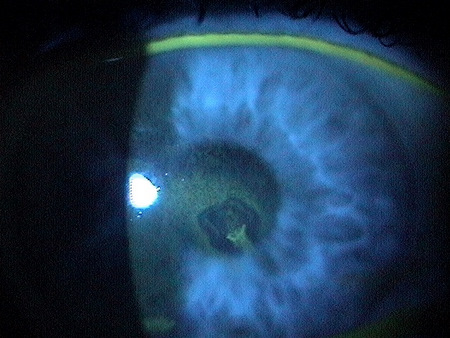
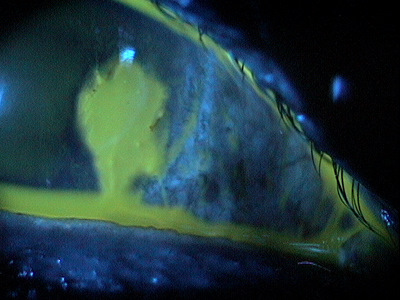
Corneal Laceration – Day 3
|
|
 |
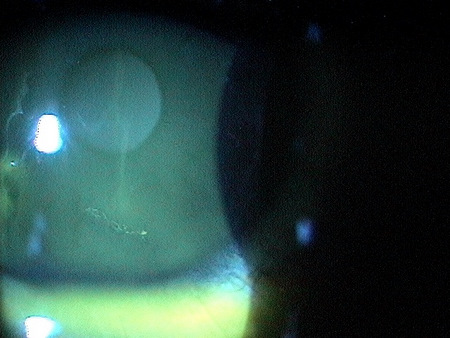
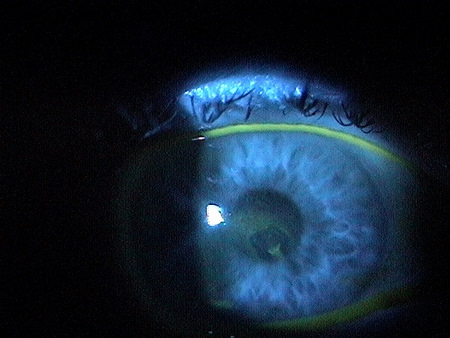
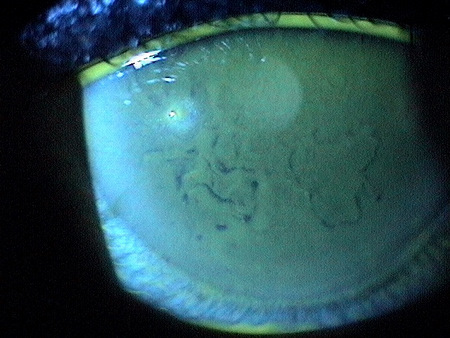
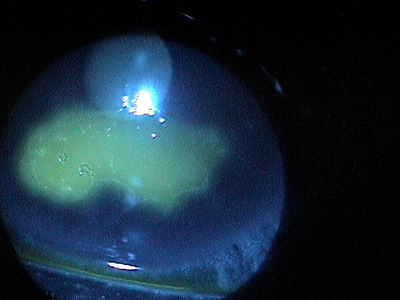
Recurrent Corneal Erosion – 6 months later
|
The main goal of the diagnostic evaluation in a patient with recurrent corneal erosion is to accomplish the following:
- Determine the underlying etiology of the corneal erosion (if possible – must directly quiz the patient about prior insult to the eye, even if years earlier)
- Relieve ocular pain and discomfort
- Prescribe a treatment program to treat the condition and prevent future occurrences
Patient History
Patients with recurrent corneal erosion may present with any of the following abnormal clinical signs and symptoms:
- Mild foreign body sensation
- Episodic tearing
- Blepharospasm
- Photophobia
- Decreased vision
- Severe ocular pain
- Characteristic discomfort to pain plus lacrimation upon waking, subsiding over minutes to hours
Adnexal Examination
- Pseudoptosis of the lid may be present during gross examination of the face and adnexa.
- Ask patient about the history of the ptosis to determine if it is a recent occurrence or has been present for a long time
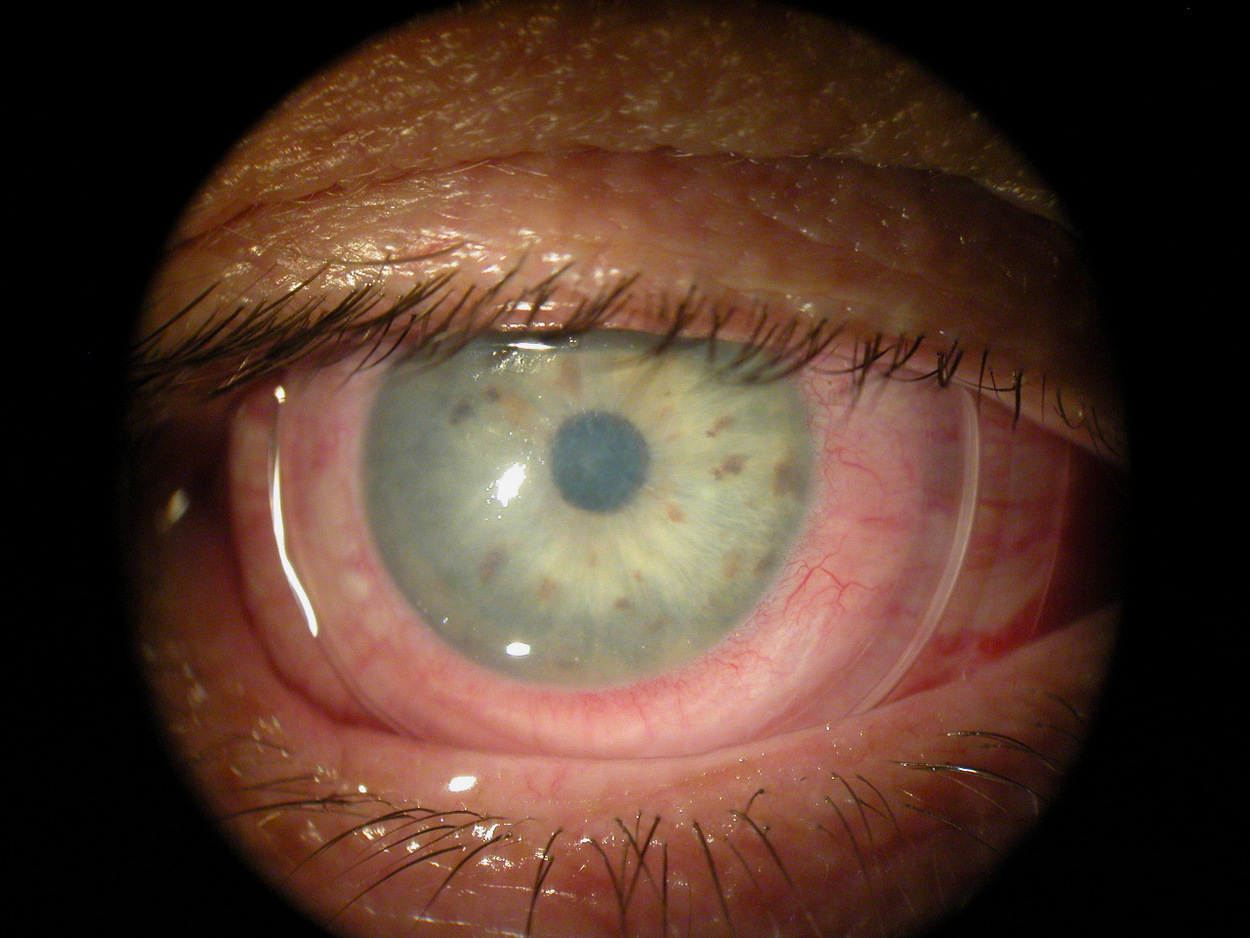
External Ocular Examination with Biomicroscopy
- Strands of tissue or debris on the corneal surface
- Defects of the corneal epithelium
- Gross epithelial sloughing
- Roughening of the corneal epithelium
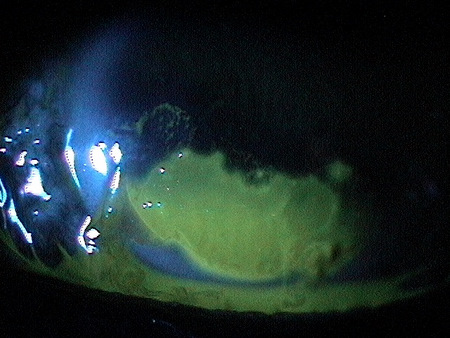
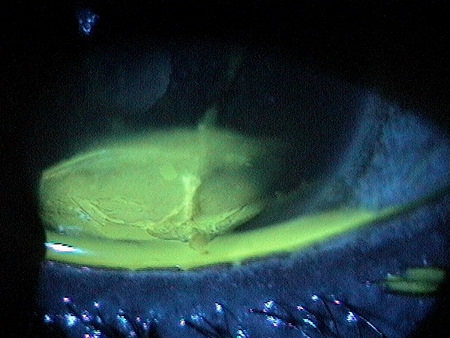
- Acute presentations will often show areas of irregular positive fluorescein staining
- Quiescent presentations will show characteristic negative staining
- Areas of negative staining can be very subtle
- Evaluation of the palbebral conjunctiva
 |
|
||
 |
|
||
 |
|
||
 |
|
||
 |
|
Extenal Ocular Photography
- Document the location and extent of the erosion on the cornea
- Document any other associated structural changes to the cornea and the eyelids
- Document the progress or lack of progress of the corneal erosion
- Document the delivery of medical treatment
- Document the response to treatment
 |
|
||
|
|
||
 |
|
Recurrent corneal erosions may be classified as either acute or chronic. Acute recurrent corneal erosion is somewhat of a misnomer. It really indicates an erosion that is presenting due to acute symptoms but the injury actually happened some time ago. A chronic presentation may or may not have symptoms but will often have a history indicating a prior erosion.
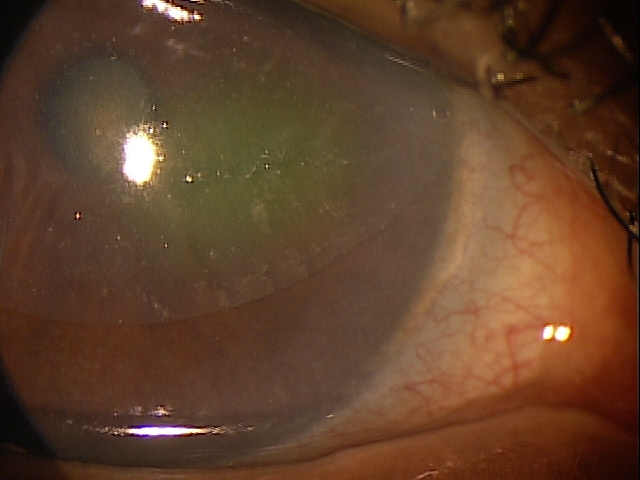
Recurrent corneal erosions may also be classified as either superficial or deep.
|
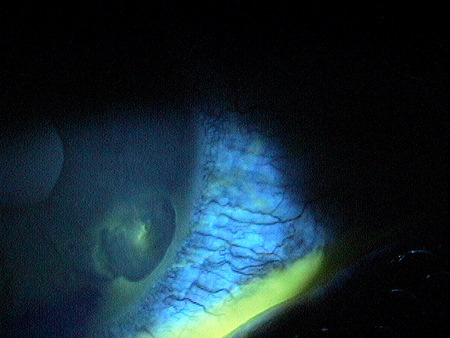
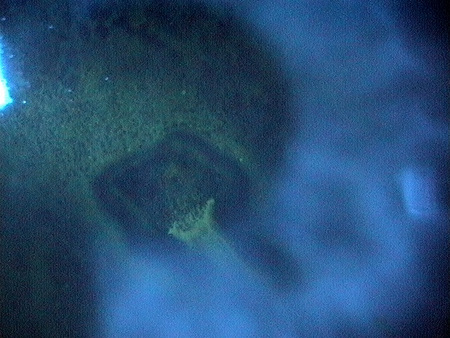
Superficial Recurrent Corneal Erosion
|
Differential diagnoses would include any corneal condition presenting with strands of tissue or debris on the corneal surface and/or a defect of the corneal epithelium.
|
 |
|||||
 |
|
|||||
Anterior Basement Membrane Dystrophy
|
 |
The goals of treating recurrent corneal erosion include the following:
- Facilitate re-epithelialization
- Reduce pain and inflammation
- Prevent secondary infection
- Prevent recurrence of the erosion
 |
|
||
 |
|
Pharmocologic Treatment
Assuming that if the patient has a stable erosion that does not require surgical intervention:
- Artificial tears four times per day (FreshKote or un-preserved tears)
- 5% hypertonic ophthalmic solution up to four times per day for several weeks
- 5% hypertonic ophtahlmic ointment at bedtime for several weeks
- Avoid lubricating ointment at bedtime
- Topical steroid eye drops three times per day for three weeks (Pred Forte 1%)
- Oral tetracycline derivatives 50mg once or twice daily for two months to inhibit matrix metalloproteinase-9 (doxycycline or minocycline)
- Pain control with topical non-steroidal anti-inflammatory eye drops (Bromday once daily)
- Mild-to-moderate recurrent corneal erosion presentations require minimal pain medication
- If the pain is significant, although they will help, very few oral pain medications can actually stop severe corneal pain
- Patients should be warned that until the cornea begins to heal, pain is undeniable
NOTE: The use of hypertonics alone in the treatment of recurrent corneal erosion is a clinical waste of time. Hypertonics do nothing to eliminate the underlying cause of the problem and only delay the inevitable and needed aggressive medical and/or surgical intervention.
Mechanical Treatment
Bandage Contact Lenses
- Bandage contact lenses are almost essential in both the acute management of recurrent corneal erosion and to aid in presenting recurrences
- In addition to the pharmacologic treatment, high DK, high modulus soft lenses should be applied and remain on the eye for extended period of time
- Continuous wear of the lenses can often last 1-2 months, depending on the severity of the initial presentation
- Lenses should not be left on longer than their approved extended wear period
- When using a bandage contact lens, hyperosmotic ointment should be avoided and a broad spectrum topical antibiotic drop prescribed twice a day simply for prophylaxis
Pressure-Patch
- Except in the cases of very extensive, almost limbus to limbus corneal erosion, bandage contact lenses are far more preferred than pressure-patching
Surgical Treatment
Consider surgical treatment options if pharmacologic and mechanical treatments are unsuccessful and corneal erosion recurrs.
Amnionic Membrane Inserts
- An excellent choice for recurrent corneal erosion treatment, again assuming the wound is managed and the basement membrane is clean
 |
ProKera Amniotic Membrane Insert
|
|
BioDOptix Amniotic Membrane Insert
|
 |
Surgical Treatment
Consider surgical treatment options if pharmacologic and mechanical treatments are unsuccessful and corneal erosion recurrs.
- Superficial keratectomy with light polish of the basement membrane with diamond burr
If the burr is used to remove all defective epithelium, the edges are contoured to create a healing edge for the healthy cornea, and the basement membrane is cleared of debris through a light polish, this technique is essentially 100% effective in eliminating any recurrences of the erosion.
- Photorefractive keratectomy
PRK is another choice, especially if the patient has an ametropic condition that could benefit from the laser application. If used soley to treat the corneal disorder, this would be best classified as a phototherapeutic keratectomy (PTK).
- Anterior stromal puncture
Despite remaining in the literature, few practitioners consider this somewhat barbaric intervention as an effective treatment tool for recurrent corneal erosion. When one considers the effective outcomes from aggressive medical treatment and the almost 100% effectiveness from a properly performed keratectomy procedure, the option to perform anterior stromal puncture seems mute.
- Alcohol delamination of the corneal epithelium may be considered for recalcitrant presentations
 |
|
||
 |
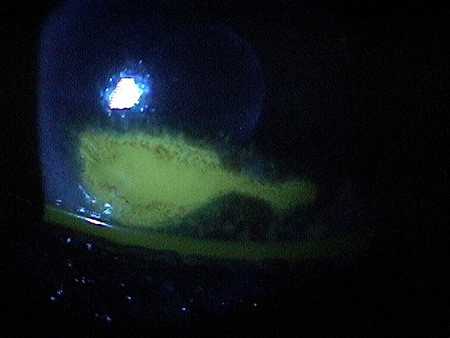
Resolving Corneal Erosion – Day 3
|
||
 |
|
1. Bronner A. Peeling Back The Layers of RCE. RevOptom. 1 Jan 2013. http://www.revoptom.com/content/c/38713/. Last accessed August 17, 2014.
2. Verma A. Recurrent Corneal Erosion Treatment and Management. 4 Aug 2014. http://emedicine.medscape.com/article/1195183-treatment. Last accessed August 17, 2014.
3. Jayaswal R. Recurrent Corneal Erosion Syndrome. Optometry Today. 6 June 2014. http://www.optometry.co.uk/uploads/articles/cet-2014/cet_2_june_6_recurrent_corneal_erosion_syndrome.pdf. Last accessed August 17, 2014.
371.42
Recurrent erosion of cornea
92285
External ocular photography
92071
Bandage contact lens
65778
Amniotic membrane placement
Occurrence
The prevalence of recurrent corneal erosion is more common in developing countries were there is lack of nutrition and in individuals with predisposing factors.
Distribution
Recurrent corneal erosions are notdistributed evenly throughout the population.
Risk Factors
- Female sex
- Age 40 and above
- History of dry eye syndrome
- History of epithelial basement membrane dystrophy
- History of corneal stromal dystrophy
- History of corneal endothelial dystrophy
- History of corneal abrasion or laceration
- History of corneal transplant surgery
- History of cataract surgery
- History of LASIK
- Diabetes