

 Print | Share
Print | Share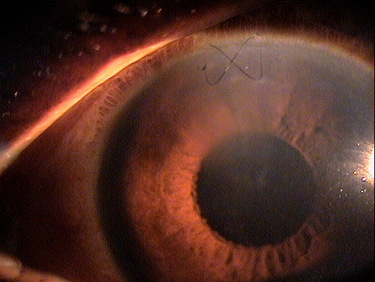
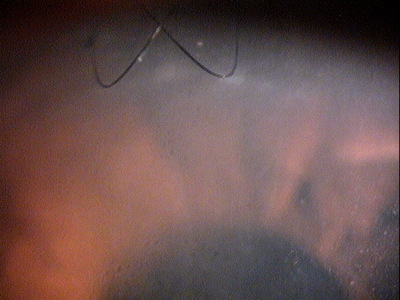
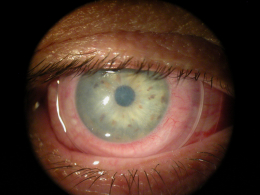
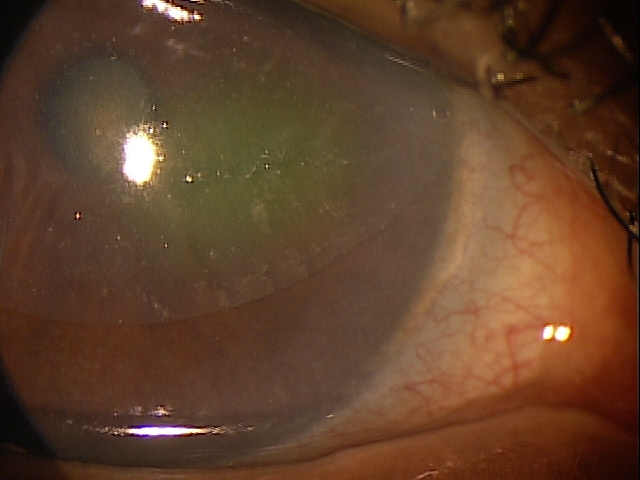
Loss of stromal transparency in the
superior region of the cornea
ICD-10 Diagnosis Codes:
H18.231–Secondary corneal edema, right eye
H18.232–Secondary cornea edema, left eye
H18.233–Seondary cornea edema, bilateral
Title
Secondary Corneal Edema
Category
Corneal Opacity And Other Disorders Of Cornea
Description
Corneal edema is not a diagnosis in itself, but rather a clinical sign of an underlying condition.
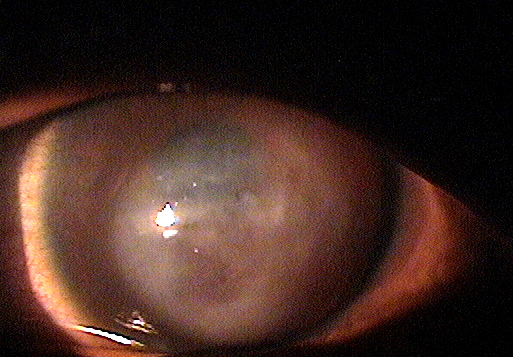
Corneal edema is a clinical sign of corneal disease. The condition is characterized by an increase in corneal thickness secondary to an abnormal accumulation of fluid. The excess fluid produces a swelling of the corneal tissue and can result in a loss of stromal transparency that produces blurred vision or visual impairment.
 |
Corneal edema may occur in any of the following conditions:
|
The layers of the cornea are optically transparent so that the entire structure can transmit visible light. When viewed in cross-section, the cornea is a basic structure of two covering layers with a central collagen stroma. The outer covering layer is called the anterior cornea. It is composed of the corneal epithelium and a basement membrane called Bowman’s membrane. This layer functions as a semi-permeable membrane that keeps pathogens out of the eye but allows nutrients from the pre-ocular tear film to nourish the anterior cornea.
The middle layer of the cornea is called the stroma. This layer comprises over 90% of the cornea’s thickness and is composed of tightly packed collagen fibrils in an orderly lamellar arrangement. The spacing and arrangement of the fibrils makes the corneal stroma optically transparent. To maintain optical transparency, the stroma must be maintained in a state of relative deturgescence and the normal level of stromal hydration is 78% water. The inability to maintain stromal deturgescenece can result in corneal edema and a loss of stromal transparency.
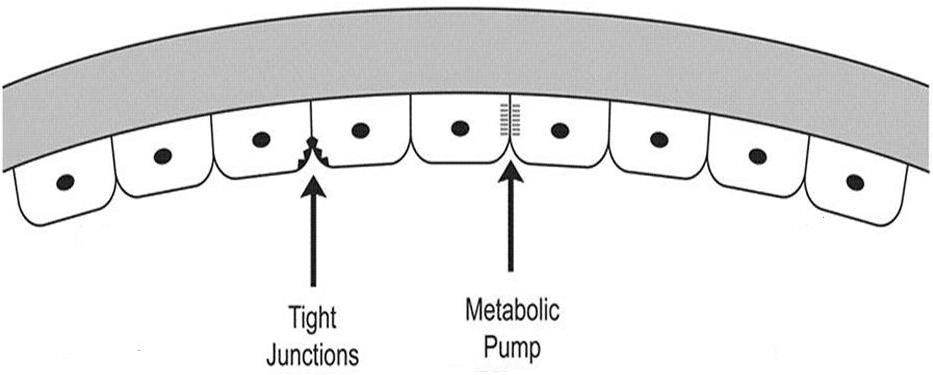
The inner covering layer is called the posterior cornea. It is composed of the corneal endothelium and Descemet’s membrane. This layer fuctions as a semi-permeable membrane that controls fluid and solute transport across the posterior surface of the cornea. Because of the strength and flexibility of Descemet’s membrane, the posterior cornea also serves as a barrier against injury.
 |
Posterior Cornea
|
|
 |
Stromal Edema
|
|
Epithelial Edema
|
 |
The main goal of the diagnostic evaluation in a patient with corneal edema is to accomplish the following:
- Determine the underlying condition producing the corneal edema
- Treat the underlying condition
- Treat the corneal edema, if necessary
Patient History
Patients will usually present with the following symptoms:
- Blurred vision
- Fluctuating vision
- Cloudy vision
- Sensitivity to bright light
- Halos around point sources of light
- Contact lens intolerance
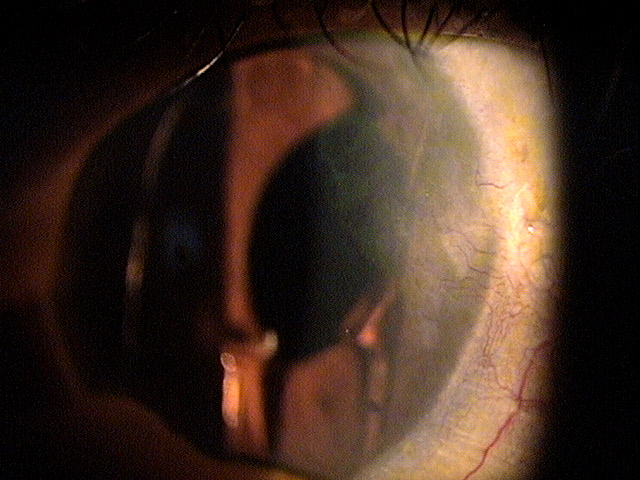
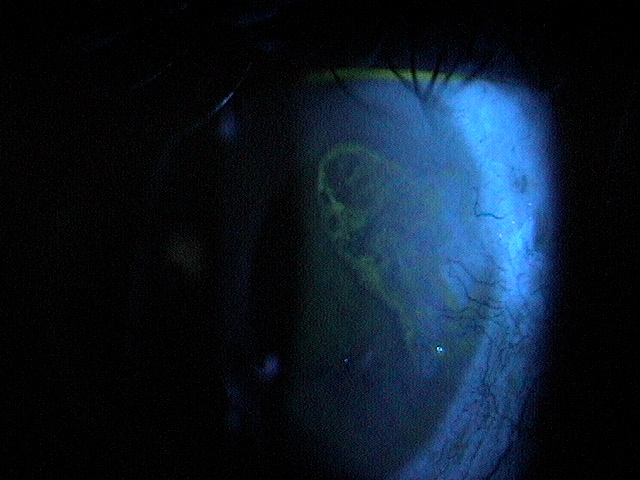
External Examination with Biomicroscopy
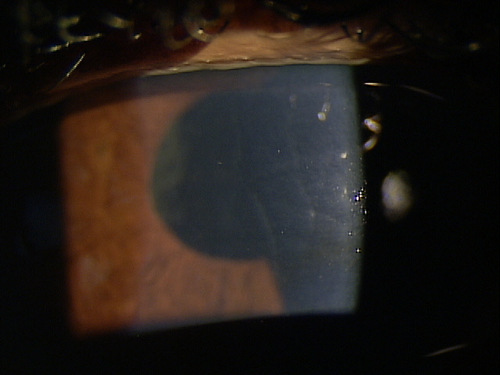
- Loss of stromal transparency
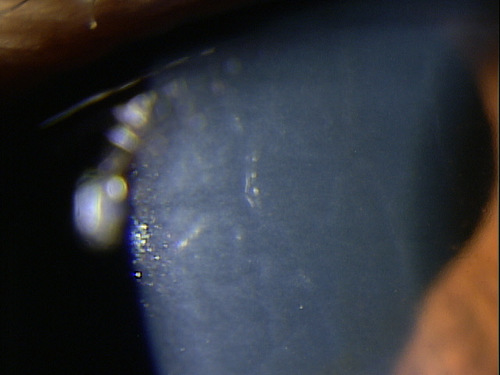
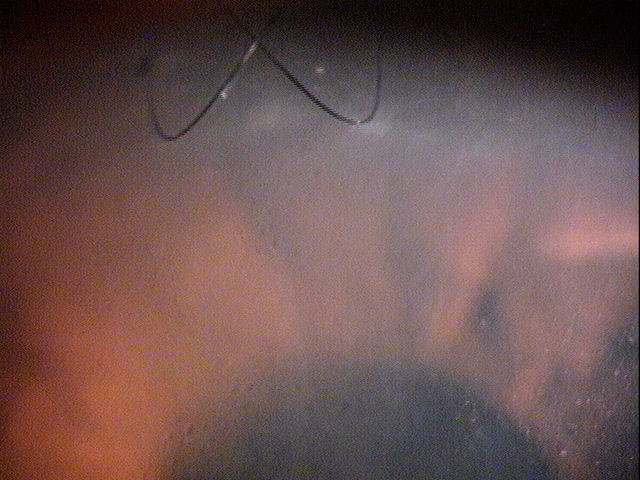
- Folds in Descemet’s membrane
- Obvious thickening of the cornea
- Corneal guttata
- Epithelial edema
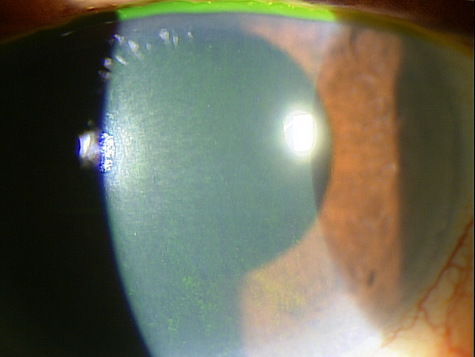 |
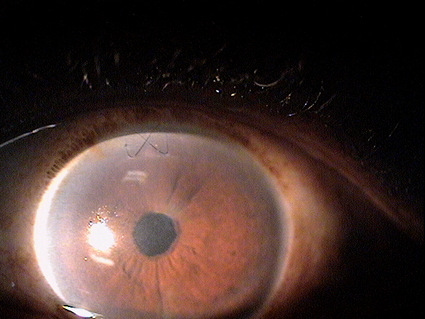
Clinical Appearance of the Cornea
|
|
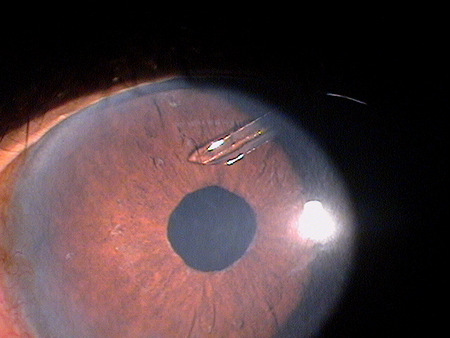 |
Clinical Appearance of the Cornea
|
|
 |
Clinical Appearance of the Cornea
|
|
 |
Clinical Appearance of the Cornea
|
|
 |
Clinical Appearance of the Cornea
|
|
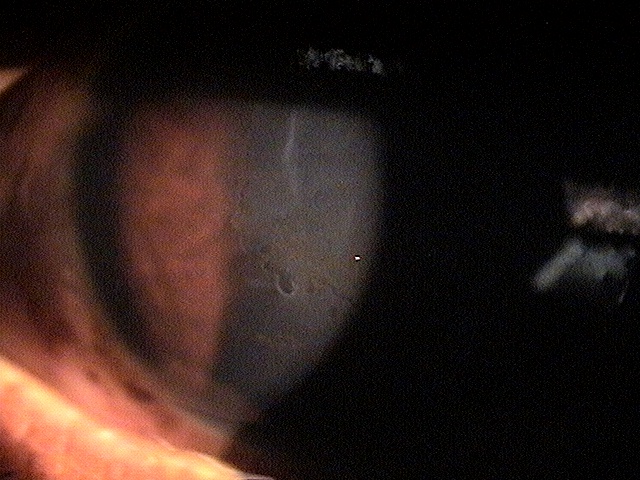 |
Clinical Appearance of the Cornea
|
|
 |
Clinical Appearance of the Cornea
|
DIAGNOSTIC TESTS
External Ocular Photography
- To document the progress or lack of progress of corneal edema
- To help plan a treatment program
- To document the delivery and response to medical treatment
 |
 |
 |
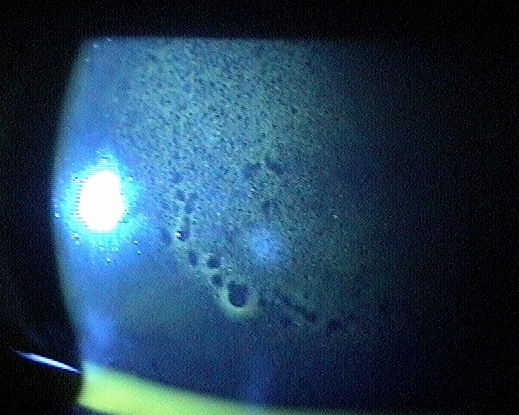
Specular Endothelial Microscopy
- To document the progress or lack of progress of corneal edema
- To visualize and analyze the corneal endothelium
- To document the progress or lack of progress of a corneal endotheliopathy
- To help plan a treatment program
- To document the delivery and response to medical treatment
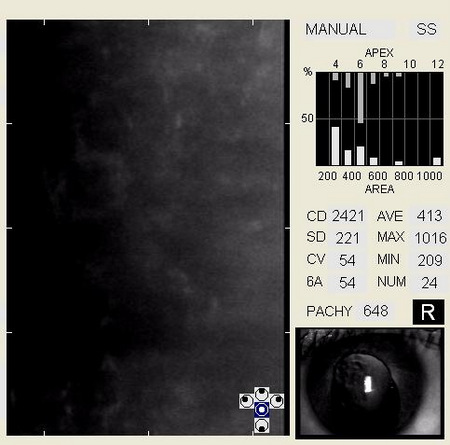 |
Specular Endothelial Microscopy
|
Congential Corneal Edema
Most cases of congenital corneal edema result from birth trauma, congenital glaucoma, or congenital hereditary corneal endothelial dystrophy. These are rarely seen in a primary eye care practice.
Acquired Corneal Edema
Acquired corneal edema may occur with many eye diseases and conditions and these include the primary and secondary corneal endotheliopathies.
| Primary Corneal Endotheliopathies | Secondary Corneal Endotheliopathies | |
|
|
Corneal edema has few conditions that mimic its appearance. A few could be:
Corneal scarring from prior injury
In this case the lack of transparency will be confined to the stromal area and likely associated with a traumatic history.
 |
Severe Corneal Edema
|
Corneal scarring from prior surgery
Focal areas of scarring can be confused with edema (i.e. scarring at an incision site from prior cataract surgery or corneal surgery – especially prior PRK or LASIK).
In both cases, scars take on a denser appearance, often have very irregular patterns unless associated with an incision site and should have a supportive history. The only differential diagnosis relates to uncovering the underlying etiology for the apparent corneal disease.
 |
 |
Because corneal edema can be caused by various eye diseases and conditions, the condition is treated according to the cause. The first goal of treating patients with corneal edema is to reduce the edema and the associated symptoms of blurred vision and ocular discomfort. Second, best practices treatment guidelines indicate treatment of the underlying condition producing the corneal edema.
Preventative Treatment
- Avoiding or minimizing contact lens wear in patients with preexisting endothelial disease or in patients with established patterns of abusive contact lens overwear
- Careful consideration before recommending cataract surgery in patients with preexisting endothelial disease
- Surgery may be delayed or a combined procedure recommended in the cases of advanced corneal compromise
Pharmocologic Treatment
Hyperosmotics
- The goal of treatment is to improve visual acuity by deturgescence of the stroma or epithelium
- Hyperosmotics have their greatest effect on epithelial edema and minimal ability to reduce stromal compromise
- Nighttime ointment use is often more effective due to the moderate to severe burning sensations associated with topcial hyperosmotic solutions in some patients
Artificial Tears (FreshKote Ophthalmic Solution)
- The goal of treatment is to remove excess water from the epithelium by utilizing the high oncotic pressure of the solution
Topical Steroids
- Since low grade ocular inflammation is associated with chronic corneal edema, topical steroids can be used in patients with both uveitis and secondary corneal edema
Topical Glaucoma Medications
- Lowering intraocular pressure can be one of the most effective means of decreasing corneal edema, especially stromal and posterior edema
- Decreasing the osmotic gradient by lowering IOP gives the endothelium a better chance of “catching up”
- Any decrease in IOP is beneficial and should be achieved with aqueous suppressant agents
Mechanical Treatment
Bandage contact lens
- In patients with epithelial edema, overnight wear of soft contact lens can be used to decrease pain and improve visual acuity
Surgical Treatment
- Amniotic membrane placement
- Endothelial transplant
- Penetrating keratoplasty
Amniotic Membrane Inserts:
 |
ProKera Amniotic Membrane Insert
|
|
BioDOptix Amniotic Membrane Insert
|
 |
1. Aquavella JV. Keratopathy, Pseudophakic Bullous. http://www.emedicine.com/oph/topic107.htm. Last accessed March 30, 2014.
2. Heiting G. Fuchs’ corneal dystrophy: 7 things you should know. http://www.allaboutvision.com/conditions/fuchs-corneal-dystrophy.htm. Last accessed March 30, 2014.
3. Corneal diseases. http://www.innvista.com/health/ailments/eye-ailments/corneal-diseases/. Last accessed March 30, 2014.
4. Ajamian PC. Warning: corneal edema ahead. RevOptom. July 2009;146(7): http://www.reviewofoptometry.com/content/d/cataract___and___refractive_surgery/c/14568/. Last accessed March 30, 2014.
5. Raizman M. Maintaining corneal barrier integrity. RevOptom. Oct 2007; 144(10).
371.22
Secondary corneal edema
92225
External ocular photography
92286
Specular endothelial microscopy
76514
Corneal pachymetry
92025
Corneal topography
92312
Anterior segment imaging
92071
Bandage contact lens
65778
Amniotic membrane placement
76513
Anterior segment ultrasound