

 Print | Share
Print | Share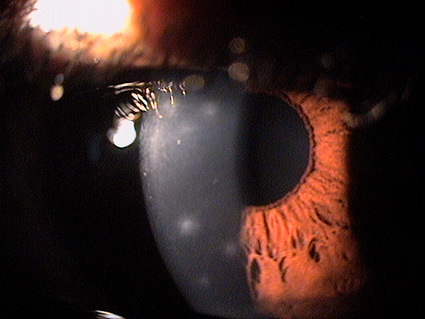
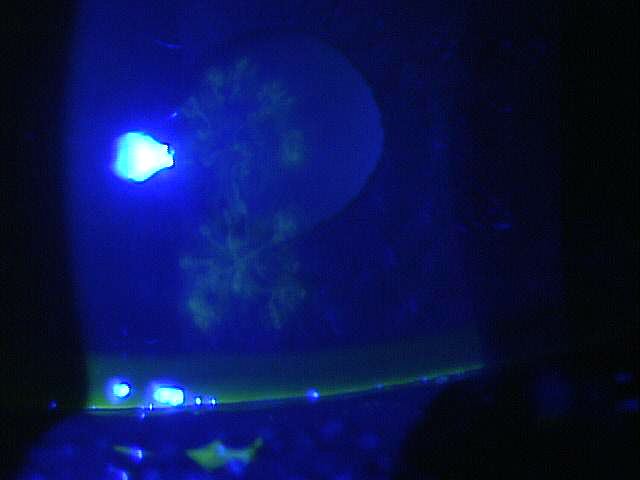
Corneal infiltrates seen in adenoviral keratoconjunctivitis
ICD-10 Diagnosis Code:
B30.0 — Keratoconjunctivitis due to adenovirus
Title
Adenoviral Keratoconjunctivitis
Category
Other Diseases Of The Conjunctiva Due To Viruses And Chlamydiae
Description
Adenoviral keratoconjunctivitis is a type of adenoviral eye infection
Adenoviruses are unenveloped viruses with a linear, double stranded DNA genome. Adenoviral keratoconjunctivitis is a clinical manifestation of adenovirus infection and is often accompanied by a variety of upper respiratory infections. Although there are over 50 adenoviral serotypes that affect humans, adenoviral keratoconjunctivitis is usually caused by serotypes 3, 7, 8, 11, 19 or 37.
Adenoviral keratoconjunctivitis is a highly contagious ocular infection. Transmission of the virus occurs because it is found in respiratory or ocular secretions, contaminated eye drop bottles, and make-up containers. The infection usually starts in one eye and progresses to the other several days later.
The incubation period for adenoviral keratoconjunctivitis is 2-14 days. In addition, the patient may remain infectious for 10-14 days after symptoms develop. Adenoviral infections may be preceded by any of the following symptoms:
- Flu-like symptoms
- Fever
- Malaise
- Respiratory distress
- Vomiting
- Diarrhea
 |
Adenoviral Keratoconjunctivitis
|
Structural Damage to the Eye
- Eyelid edema
- Inferior conjunctival palpebral follicles
- Conjunctival hyperemia
- Conjunctival chemosis
- Conjunctival hemorrhage
- Conjunctival pseudomembrane
- Punctate corneal epitheliopathy
- Corneal infiltrates in the anterior to mid-stroma
- Negative corneal staining associated with elevated corneal infiltrates
Functional Damage to the Eye
- Decreased visual acuity can occur as a result of the compromised corneal epithelium
- Decreased visual acuity can occur as a result of opaque corneal infiltrates in the visual axis
The main goal of the diagnostic evaluation in a patient with adenoviral keratoconjunctivitis is to accomplish the following:
- To establish the diagnosis of adenoviral keratoconjunctivitis before the patient leaves your office
- To educate the patient so that he/she avoids contaminating others
- To prescribe appropriate therapy
- Reduce unnecessary antibiotic prescriptions
- Help prevent antibiotic resistance
To obtain the information required to determine a clinical diagnosis of adenoviral keratoconjunctivitis and prescribe a treatment program, the following service components of a medical eye examination should be performed:
- Patient history
- General medical observation
- Adnexal examination
- External ocular examination with biomicroscopy
Patient History
Patients with adenoviral keratoconjunctivitis may present with any of the following abnormal signs or symptoms:
- Red eyes
- Ocular itching
- Ocular discomfort
- Foreign body sensation
- Watery eyes
- Photophobia
- Eyelid edema
- Preauricular lymphadenopathy
External Ocular Examination with Biomicroscopy
Evaluate the eyelids, conjunctiva, and cornea.
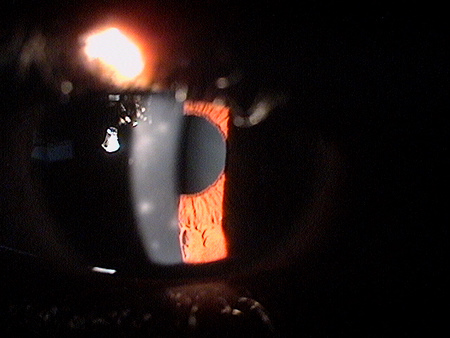 |
Clinical Appearance of the Cornea
|
|
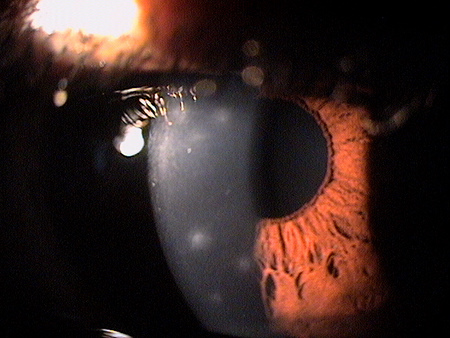 |
Clinical Appearance of the Cornea
|
|
 |
Clinical Appearance of the Cornea
|
Adenoviral Conjunctivitis
The milder form of the disease usually presents with unilateral redness, epiphora, photophobia, and ocular discomfort. The fellow eye is usually affected one to two days later with a milder presentation.
- Eyelid edema
- Tender preauricular lymph node
- Follicular conjunctivitis
- Pseudomembranous conjunctivitis
Adenoviral Keratitis
The more severe form of the disease involves the cornea and can result in permanent visual impairment.
- Punctate epithelial keratitis
- Subepithelial infiltrates
- Permanent corneal opacities
Because the spectrum of adenoviral eye infection varies from sub-clinical disease to serious infection, a rapid screening procedure is a cost-effective way to exclude differential diagnoses and avoid unnecessary treatment with topical antibiotics. In-office screening can be done with the Rapid Pathogen Screening (RPS) AdenoPlus Detector, a lateral flow immunoassay testing device that takes about ten minutes to perform.
Contact Lens Wear
Infiltrates and ocular redness associated with contact lens wear should be differentiated from those caused by adenoviruses. For example, contact lens-related infiltrates are generally less severe and resolve faster. Corneal infiltrates produced by adenoviral infection generally appear one to two weeks after the onset of symptoms.
Chlamydial Infections / Bacterial Infections
These conditions can present with corneal infiltrates similar to those found in adenoviral disease.
Rosacea
Corneal disease secondary to ocular rosacea may produce punctate epithelial erosions that are similar in appearance to corneal infiltrates.
The key to treating adenoviral keratoconjunctivitis is making the correct diagnosis. Treatment options vary depending upon the severity of the disease.
Palliative Treatment
- Artificial tears and cold compresses until spontaneous resolution occurs (e.g., up to 3 weeks)
Pharmacologic Treatment
- Topical decongestant/anti-histamine for severe itching
- Topical steroids for severe membraneous conjunctivitis
- Topical steroids for subepithelial infiltrates
- Topical antiviral agents (i.e., off-label use of Zirgan ophtahlmic gel)
Because steroids only suppress the corneal inflammation as long as they are used, a prolonged taper is recommended to prevent recurrence of the infiltrates.
Mechanical Treatment
- Patients wearing contact lenses should discontinue contact lens wear until the condition resolves
Preventative Treatment
- Frequent hand washing while the disease is active
- Avoid contact with infected individuals
- Restrict access to work and school during the first 10-12 days of the infection
- Avoid sharing bedding, towels, make-up, or any objects that may come in contact with the eye
1. Udeh BL, Schneider JE, Ohsfeldt RL. Cost effectiveness of a point-of-care test for adenoviral conjunctivitis. Am J Med Sci. 2008 Sep;336(3)0:254-64.
2. Bawazeer A. Epidemic Keratoconjunctivitis Treatment and Management. Available at http://emedicine.medscape.com/article/1192751-overview. Last accessed February 20, 2014.
3. Bowling E. Russell GE. Shovlin JP. Sindt CW. Adenoviral conjunctivitis. RevOptom: The Corneal Atlas. 2009 Jan: 5.
4. Dunbar MT. Infectious ulcer or sterile infiltrate? Rev of Cornea & Contact Lenses. 2007 Oct: 16-20.
5. Shovlin JP. Corneal infiltrates. Rev of Cornea & Contact Lenses. 2007 Oct: 6.
077.1
Adenoviral keratoconjunctivitis
92285
External ocular photography
87809QW
Infectious agent antigen detection