

 Print | Share
Print | Share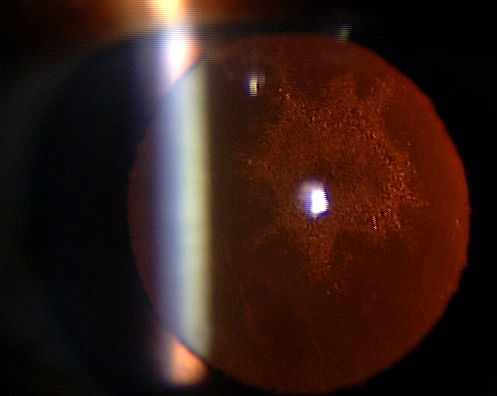
ICD-10 Diagnosis Codes:
H25.041–Posterior subcapsular polar senile cataract, right eye
H25.042–Posterior subcapsular polar senile cataract, left eye
H25.043–Posterior subcapsular polar senile cataract, bilateral
Title
Posterior Subcapsular Polar Senile Cataract
Category
Cataract
Description
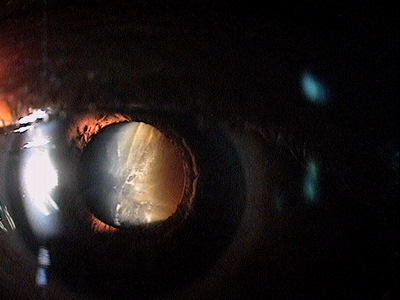
A posterior polar cataract is a round, discoid, opaque mass (see the image below) that is composed of malformed and distorted lens fibers located in the central posterior part of the lens
Posterior subcapsular polar senile cataract is a disease characterized by:
- Peroxidation of lens proteins leading to decreased transparency
- Compression of lens fibers from continued lens growth
- Accumulation of urochrome pigments from amino acid breakdown leading to brunescence
- A gradual, progressive thickening of the lens
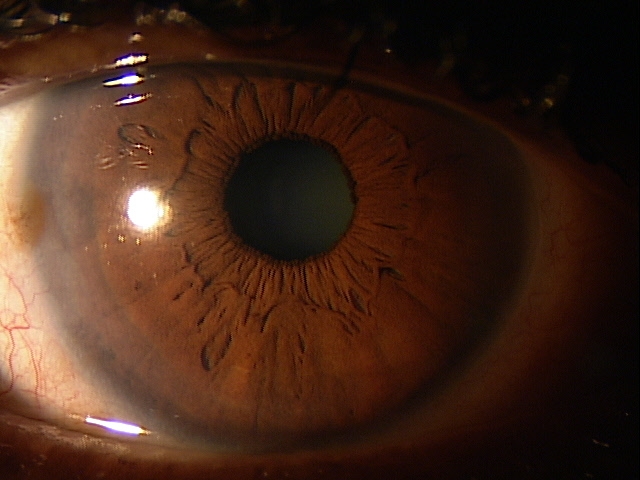 |
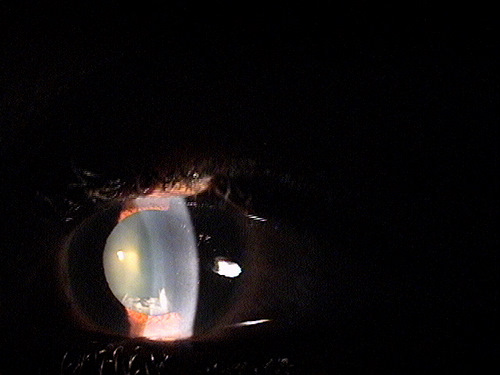
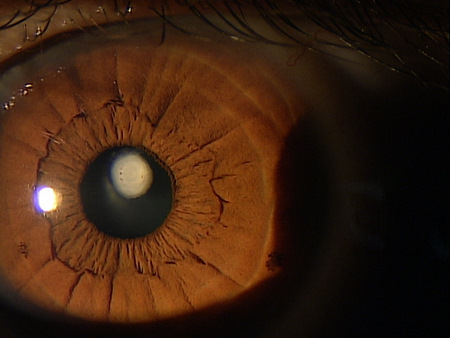
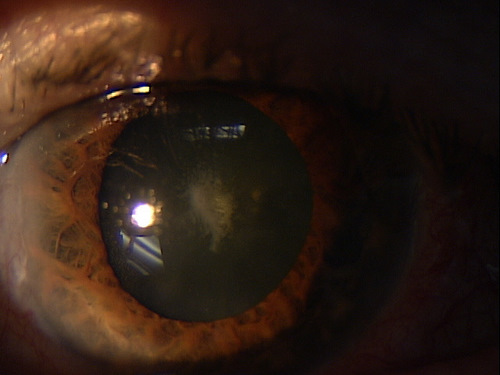
Clinical Appearance of the Lens
|
Structural Damage to the Eye
- With age, the lens changes in weight, transparency and thickness
- With age, the accommodative power decreases
- Excessive lens thickening can lead to pupillary block and secondary glaucoma (cataract surgery has shown to reduce IOP 4-6 mm Hg and sometimes much more, often eliminating the need to prescribe second medications or any other kind of additional treatment in patients with closed-angle glaucoma
Functional Damage to the Eye
- Blurred vision
- Decreased visual acuity
- Glare
- Myopic shift
- Monocular diplopia
- Patients reports seeing shadows in eye or feels their glasses are always dirty and they have to clean them all the time
The main goal of the diagnostic evaluation in a patient with posterior subcapsular cataract is to accomplish the following.
- Evaluate the level of vision impairment and determine if daily activities are affected
- Rule out or make an attempt to quantify comorbidities that could be contributing to reduced vision
Patient History
Abnormal symptoms generally include the following:
- Decreased vision
- Increase in glare
- Difficulty in daily task
- Difficulty manuvering around in dim lighting
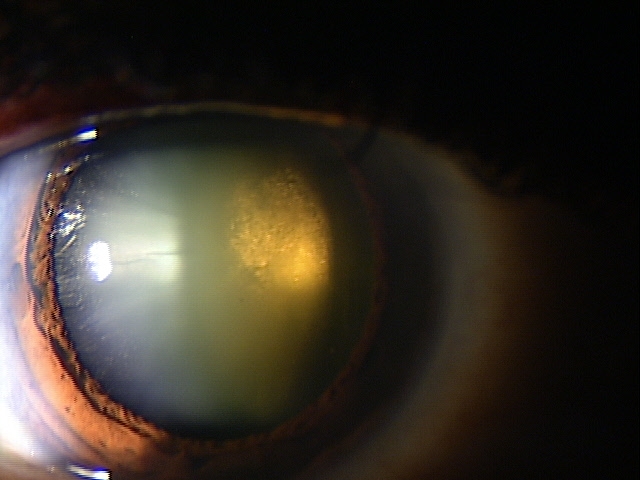 |
Clinical Appearance of the Lens
|
|
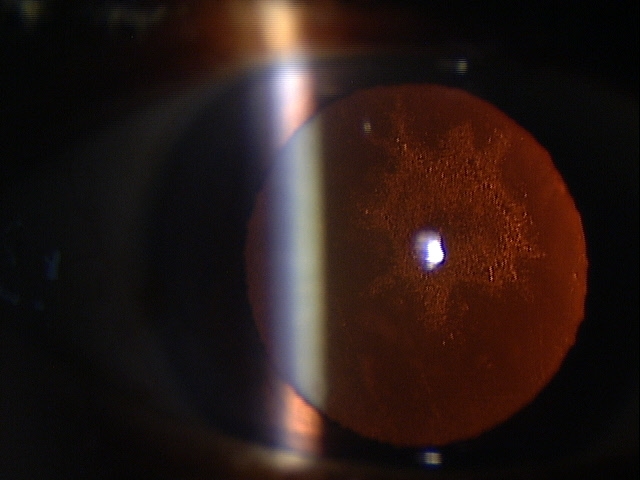 |
Clinical Appearance of the Lens
|
Senile cataracts are classified into three main types: nuclear cataract, cortical cataract, and posterior subcapsular cataract.
 |
Nuclear Cataract
|
|
Cortical Cataract
|
 |
|
 |
Anterior Subcapsular Cataract
|
Posterior Subcapsular Cataract
|
 |
None. It is important to identify any other abnormalities that could be contributing to loss of functional vision. If identified, every attempt should be made to quanitfy that effect. While the existence of comorbidities does not rule out the need for or recommendation of cataract surgery, it is necessary to make as accurate prediction as possible of the resultant postoperative acuity if the patient elects to undergo cataract surgery.
The most common age-related comorbidities to rule out are:
- Macular degeneration
- Diabetic macular edema
- Corneal dystrophies and degenerations
- Glaucoma
- Neurologic disorders
As stated, simply the presence of another cause of functional vision loss does not lessen the value of cataract surgery. One of the best examples of this scenario would be a patient with advanced cataract and moderate to advanced macular degeneration. While many physicians concentrate on the macular pathology, elimination of a significant lens opacity can dramatically improve the quality of the patient’s remaining vision.
Surgical Treatments
1. Monofocal intraocular lens
Tecnis IOL (AMO)
- Provides vision for distance only
- Designed with a prolate surface to introduce negative spherical aberration to decrease or eliminate positive spherical aberrations from the eye
- Design also helps increase contrast sensitivity especially at night
SofPort AO (Bausch & Lomb)
- Provides vision for distance only
- Designed with a prolate surface to introduce neutral spherical aberration, leaving the patient with the normal corneal spherical aberration for their age
- This design does not improve contrast sensitivity
- Design makes the lens less dependent on surgical technique or perfect centration
AcrySof IQ (Alcon)
- Provides vision for distance only
- Designed with a prolate surface to introduce negative spherical aberration to decrease or eliminate positive spherical aberrations from the eye
- This design also helps increase contrast sensitivity especially at night
- Has a transparent yellow color that does not alter the color or quality of the environment when inserted in the eye
2. Multifocal intraocular lens
Crystalens HD (Bausch & Lomb)
- Hinged design allows the lens to change position inside the eye as the patient looks at a near target
- Only FDA approved accommodative lens
- Good distance and intermediate ranges with the lens
- Limited near range (add of 1.50D to 2.00D)
- Patient occasionally to very likely will need reading glasses for small or detailed near tasks
Tecnis Multifocal (AMO)
- Diffractive design with designate zones of near, intermediate and distance
- New design is not affected by pupil size in various lighting conditions
- Shaped to correct for certain high order aberrations which improve the ability to see contrasting objects especially
ReZoom (AMO)
- Designed with alternating refractive zones that correct for either distance or near. Central optical zone corrects for distance, then near and alternating back to distance again
- Good distance, but glare may be an issue at night
AcrySof ReSTOR (Alcon)
- Designed with the principle of apodization or a series of graduated steps that result in diffraction of light at distance and near
- Two adds available (+4.00D and +3.00D)
AcrySof IQ ReSTOR (Alcon)
- Similar to the AcrySof ReSTOR except for new aspheric design helps reduce potential for glare/halos and improves contrast sensitivity
AcrySof Toric (Alcon)
- For patents with small amounts of corneal cylinder (1.00D to 1.50D) limbal relaxations incisions work well with the spherical multifocal lens
- The toric multifocal lens corrects up to 3.00D of cylinder
- Patients with cylinder greater than 3.00D can have the toric multifocal implanted with additional procedure like limbal relaxing incisions or refractive laser procedures to completely correct for the astigmatism
AcrySof IQ Toric (Alcon)
- Similar to the AcrySof Toric except for new aspheric design helps reduce potential for glare/halos and improves contrast sensitivity
AcrySof Natural (Alcon)
- Designed to filter out ultraviolet and high-energy blue light
- Has a transparent yellow color that does not alter the color or quality of the environment when inserted in the eye
It is imperative that the patients primary eye care provider, usually their optometrist, be intimately involved in the decision regarding the proper lens for that patient. The patients primary eye care provider is more atuned to the patients specific vision needs, the flexibility in their vision/perception system, and the ease at which they adapt to visual change.
1. Dahl, A. Cataracts. MedicineNet. http://www.medicinenet.com/cataracts/article.htm. Last accessed November 16, 2014.
2. Facts About Cataract. National Eye Institute. National Institutes of Health. Sept 2009. https://www.nei.nih.gov/health/cataract/cataract_facts. Last accessed November 16, 2014.
366.14
Posterior subcapsular
polar senile cataract
76519
Ophthalmic biometry by A-scan with
intraocular lens power calculation
92136
Ophthalmic biometry by
partial coherence
interferometry with intraocular
lens power calculation
92283
Color vision examination
Occurrence
- The prevalence of senile nuclear cataracts is almost 66% of the population over 75 years old
- The prevalence of senile cortical and senile posterior subcapsular cataract is about 28% and 20% respectively
Distribution
- Cataracts are distributed evenly throughout the population
Risk Factors
- Advancing age
- Increased sun exposure to eyes without UV protection
- Cigarette smoking